![]()
[2026] Get Top-Rated NCC EFM Exam Dumps Now
Passing Key To Getting EFM Certified Exam Engine PDF
NEW QUESTION # 26
A 30-minute tracing with moderate variability, accelerations, and one variable deceleration would be classified as:
- A. Category I
- B. Category II
- C. Category III
Answer: B
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NICHD/NCC criteria:
Category I must have ALL of the following:
* Baseline 110-160 bpm
* Moderate variability
* No late or variable decelerations
* Early decelerations may be present or absent
* Accelerations may be present or absent
Because this tracing has one variable deceleration, it fails Category I criterion ("no late or variable decelerations").
Category III requires:
* Absent variability with recurrent late decels, recurrent variables, or bradycardia, or
* Sinusoidal pattern
Those findings are not present.
Therefore, any tracing that:
* Has moderate variability and accelerations,
* But includes a variable deceleration, and
* Does not meet Category III criteria
...falls into the Category II (indeterminate) group.
Correct classification: B. Category II.
References:NCC C-EFM Candidate Guide; NICHD Three-Tier FHR Interpretation System; AWHONN FHMPP; Menihan; Simpson & Creehan.
NEW QUESTION # 27
This external tracing is from a 19-year-old (G1P0) at 39-weeks gestation. She is 6 cm dilated, 100% effaced, and -2 station. The fetus is in an occiput posterior position. She rates her pain as 8. She reports being lightheaded. She is most likely at risk for respiratory: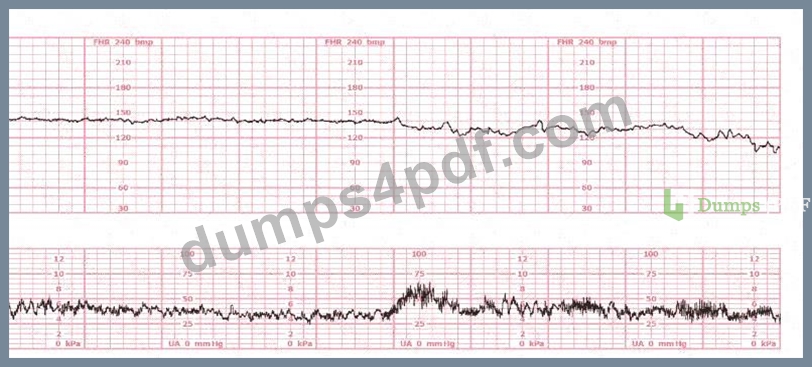
- A. Alkalosis
- B. Acidosis
- C. Depression
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Physiologic References:
This strip shows:
* Baseline around 150 bpm
* Moderate variability
* No decelerations
* Consistent, strong contractions
* A maternal report of severe pain (8/10) and feeling lightheaded
In labor, severe pain + anxiety + hyperventilation commonly cause maternal respiratory alkalosis.
NCC and AWHONN physiology guidance explain:
* Hyperventilation # # PaCO# # respiratory alkalosis
* Symptoms include:
* Lightheadedness
* Tingling
* Dizziness
* Sometimes palpitations
* This frequently occurs during painful contractions, especially with occiput posterior labor, which is notoriously more painful due to back pressure.
Why other answers are incorrect:
* A. Respiratory acidosis occurs with hypoventilation-not present here.
* C. Respiratory depression occurs with opioids, magnesium sulfate, or anesthesia-not part of this scenario.
Therefore, the correct answer is B. Alkalosis.
References:NCC C-EFM Candidate Guide; AWHONN FHMPP; Menihan EFM; Miller's Pocket Guide; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 28
The decelerations seen in the fetal monitoring tracing shown are best described as: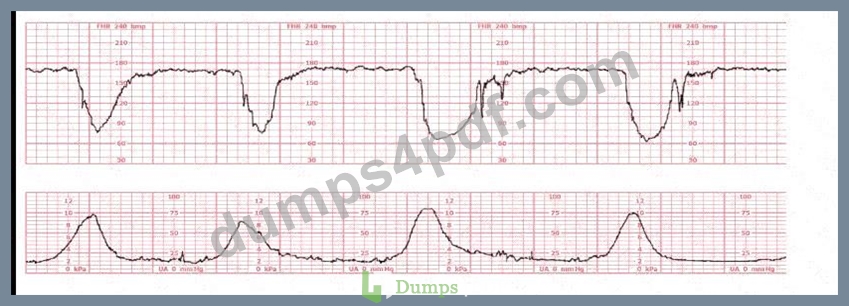
- A. Late
- B. Variable
- C. Early
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
Accurate classification of decelerations requires evaluating their shape, onset, nadir, recovery, relationship to contractions, and variability characteristics. NCC uses the NICHD standardized definitions, reinforced across AWHONN, Miller's Pocket Guide, Menihan, Simpson, and Creasy & Resnik.
Key features in this tracing:
* Abrupt onsetThe FHR drops rapidly from baseline to nadir in less than 30 seconds-this is the defining hallmark of a variable deceleration per NICHD.
* Sharp V-shape and deep amplitudeThe tracing shows steep descents and ascents, characteristic of cord compression-type variable decelerations.
* Inconsistent timing with contractionsThe decelerations do not begin at the start of contractions (as early decelerations would) and do not consistently begin after the peak of contractions (as late decelerations would). Variable decelerations can occur before, during, or after a contraction-exactly what is demonstrated here.
* Rapid return to baselineAnother core feature of variable decelerations in NICHD/NCC definitions.
* No uniform contraction relationshipEarly decelerations are symmetrical and mirror contractions.
Late decelerations begin after the peak of the contraction. This strip does not match either pattern.
Differentiation per NCC-aligned definitions:
* Early Decelerations:Gradual onset (>30 sec), nadir mirrors contraction peak, shallow, uniform.Not present.
* Late Decelerations:Gradual descent, nadir after contraction peak, smooth shape.Not present.
* Variable Decelerations:Abrupt onset (<30 sec), variable timing, sharp V-shape, rapid recovery, often with shoulders.Exactly matches the tracing.
Therefore, according to NICHD/NCC criteria, the decelerations shown are variable decelerations.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD Standardized Definitions; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 29
A woman reports 12 fetal movements over one hour. The best recommendation is to:
- A. Instruct her to count again the next day
- B. Administer a nonstress test
- C. Continue to monitor for one hour
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC and AWHONN consider fetal movement counts normal when:
* #10 distinct movements occur within 2 hours
* Or #4 movements in 1 hour for certain protocols
* Or #10 movements in 1 hour (common triage threshold)
This patient reports 12 movements in 1 hour, which is reassuring and requires no further testing.
Thus, recommending she continue daily kick counts at home is appropriate.
Why the other options are incorrect:
* A. NST is not needed because movements are normal.
* B. Continue to monitor is unnecessary; the test is already reassuring.
Correct choice: C. Count again the next day.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Assessment guidelines; Simpson & Creehan.
NEW QUESTION # 30
A fetal heart rate tracing is abnormal. A change in maternal position and oxygen administration do not correct the pattern. Following birth, a fetal cord blood sample is taken:
pH = 7.25
PaCO# = 46 mm Hg
PaO# = 20 mm Hg
HCO# = 22 mEq/L
Base deficit = -4 mEq/L
These results are best interpreted as:
- A. Hypoxia
- B. Acidosis
- C. Normal
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Normal umbilical arterial values per NCC/AWHONN/Menihan:
* pH: 7.20-7.30
* PaCO#: 45-55 mmHg
* HCO#: 20-24 mEq/L
* Base deficit: 0 to -5 (normal to mild respiratory changes)
This sample shows:
* pH 7.25 # normal
* Base deficit -4 # no metabolic acidosis
* HCO# normal
* Slightly elevated PaCO#, consistent with mild respiratory influence but still normal
* PaO# 20 mmHg is normal for cord arterial blood
This profile is not acidotic (acidosis requires pH <7.10 and base deficit #12).
It also does not indicate hypoxia, which would present with metabolic acidosis.
Therefore: Normal.
References:NCC C-EFM Candidate Guide; AWHONN FHMPP; Menihan; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 31
The baseline heart rate of a 28-week fetus is 170 bpm. The next step is to:
- A. Perform a biophysical profile
- B. Continue observation
- C. Assess maternal vital signs
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract Without Any URLs or Links:
NCC references (AWHONN, Simpson, Menihan) and the Physiology domain emphasize that baseline fetal heart rate is higher at earlier gestational ages due to predominant sympathetic tone and immature parasympathetic modulation. For a 28-week fetus, a baseline between 150-170 bpm may fall within the upper normal/mild tachycardic range.
Before classifying fetal tachycardia, recommended by AWHONN and Simpson, clinicians must first assess maternal contributors:
* Fever
* Tachycardia
* Infection
* Dehydration
* Medications (e.g., beta-agonists)
* Anxiety
This matches NCC's required first-line action: evaluate maternal status before escalating fetal assessment.
A biophysical profile (BPP) is not the immediate next step unless maternal status and fetal environment do not explain the finding. Continuing observation without maternal evaluation is contrary to perinatal safety standards.
References:AWHONN Fetal Monitoring PrinciplesSimpson & Miller Fetal MonitoringMenihan EFM Interpretation GuideNCC C-EFM Exam Content Domains 2025
NEW QUESTION # 32
A nulliparous woman at term presents with leaking fluid. Rupture of membranes confirmed. After 6 hours she is completely dilated, +2 station, has been pushing 2 hours with oxytocin at 10 mU/min. The fetal tracing is shown. What is the next step in management?
- A. Decrease oxytocin
- B. Expedite birth
- C. Continue pushing for another hour
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract Without Any URLs or Links:
According to the NCC C-EFM 2025 Exam Content Outline and recommended references such as AWHONN Fetal Heart Monitoring Principles, Simpson & Miller (Fetal Monitoring Text), and Menihan's EFM Guide, recurrent variable or late decelerations with minimal or moderate variability during the second stage of labor-particularly when the patient has been pushing for #2 hours-indicate progressive fetal intolerance of labor.
AWHONN states that when the fetal tracing displays recurrent variable decelerations with ongoing stress from long second stage, the recommended intervention is operative or expedited vaginal birth, provided the fetal station is at +2 or lower. AWHONN and Simpson emphasize that reducing oxytocin is insufficient when the tracing demonstrates ongoing significant decelerations during active pushing with adequate descent.
The NCC blueprint within Pattern Recognition & Intervention emphasizes:
* Identifying worsening recurrent decelerations
* Acting when fetal tolerance is decreasing
* Prioritizing timely intervention when the second stage exceeds standard limits with a non-reassuring tracing Because she is fully dilated, vertex at +2, and tracing shows recurrent decelerations during pushing, the evidence-based next step is expediting birth, typically via operative vaginal delivery.
References:AWHONN Fetal Heart Monitoring Principles & PracticesSimpson & Miller: Fetal MonitoringMenihan: Electronic Fetal MonitoringNCC C-EFM Exam Content Outline 2025
NEW QUESTION # 33
Patient safety is enhanced when alarms:
- A. Occur infrequently
- B. Are determined by the unit leaders
- C. Can be called by anyone
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC and AWHONN emphasize unit-wide shared responsibility for:
* Recognizing abnormal maternal or fetal findings
* Calling for help
* Triggering emergency responses (e.g., unit huddle, rapid response, safety pathways) Safety culture requires:
* Any staff member (RN, tech, provider) to initiate an alarm or escalate concern
* No hierarchy delay
* Rapid action when fetal compromise is suspected
Why the other answers are wrong:
* A. Determined by unit leaders # incorrect; safety is team-wide, not hierarchical.
* C. Occur infrequently # false; alarms must occur whenever needed, not limited.
Correct answer: B. Can be called by anyone.
References:NCC Professional Issues Domain; AWHONN Standards for Professional Practice; Perinatal Safety Bundles; Simpson & Creehan.
NEW QUESTION # 34
Maternal-fetal exchange during labor is diminished by:
- A. Placental calcifications
- B. An increase in maternal cardiac output
- C. Open-glottis pushing in second stage
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Placental calcifications:
* Reduce surface area for maternal-fetal gas exchange
* Impair placental perfusion
* Are associated with post-dates and chronic insufficiency
* Decrease the placenta's ability to oxygenate the fetus
Why the incorrect answers are wrong:
* A. Increased maternal cardiac output # improves uteroplacental perfusion.
* B. Open-glottis pushing # improves oxygenation compared with closed-glottis Valsalva pushing.
Correct answer: Placental calcifications.
References:NCC Physiology Domain; Creasy & Resnik; Simpson & Creehan; AWHONN FHMPP.
NEW QUESTION # 35
(Full question statement)
The American College of Obstetricians and Gynecologists (ACOG) recommends continuous electronic fetal monitoring in pregnancies when there is:
- A. Maternal diabetes
- B. A history of preterm birth
- C. Macrosomia
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract Without Links:
NCC relies heavily on ACOG Practice Bulletins for risk-based monitoring decisions. ACOG identifies maternal diabetes (pregestational or poorly controlled gestational diabetes) as a key high-risk obstetric condition warranting continuous electronic fetal monitoring due to risks such as fetal hypoxia, macrosomia, and metabolic complications.
In contrast, a history of preterm birth does not necessarily require continuous monitoring unless current pregnancy complications are present.
Macrosomia alone does not automatically justify continuous EFM unless accompanied by other risk factors.
Therefore, according to NCC-aligned ACOG clinical criteria, maternal diabetes is the correct indication.
NEW QUESTION # 36
A woman at 41-weeks gestation is being induced. She is 2 cm dilated and is on oxytocin at 8 milliunits
/minute. Based on the fetal heart rate tracing shown, the best initial response is to: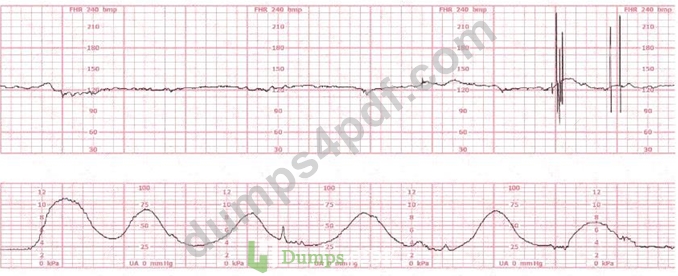
- A. Place a fetal spiral electrode
- B. Decrease the oxytocin
- C. Continue to observe
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The tracing shows tachysystole with emerging late decelerations and minimal variability:
* 5 contractions in 10 minutes
* Deceleration nadirs occur after the peak of the contraction (late pattern)
* Variability begins to trend toward minimal
* The tracing has deteriorated while on oxytocin 8 mU/min, a common threshold for overstimulation NCC and AWHONN emphasize that when tachysystole occurs with any fetal intolerance, the first action is to reduce or stop oxytocin.
Key NCC principles:
* Late decelerations + tachysystole = uteroplacental insufficiency caused by excessive uterine activity
* Interventions:
* Stop or reduce oxytocin
* Maternal repositioning
* IV fluid bolus
* Possible oxygen if other measures fail
Why the other options are incorrect:
* A. Continue to observe - not acceptable with late decels + tachysystole.
* C. Place a spiral electrode - this corrects signal quality, not uterine overstimulation or fetal oxygenation.
Thus, the best initial response is B. Decrease the oxytocin.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; NICHD Definitions; Miller & Menihan EFM texts; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 37
When a difference in interpretation occurs over a non-emergent electronic fetal heart rate tracing, the first step toward resolution is to:
- A. Have the involved clinicians review the tracing together
- B. Document the incident in the medical record
- C. Follow the chain of command
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC's Professional Issues domain emphasizes communication, collaboration, and team-based interpretation of electronic fetal monitoring tracings.
For non-emergent differences in interpretation, the first step is:
* Discussion and joint review of the tracing by the involved clinicians.
Only if disagreement persists should the chain of command be used. Documentation occurs after consensus or escalation-not as the first step.
Thus, the appropriate first step is C. Have the involved clinicians review the tracing together.
References:NCC C-EFM Candidate Guide; AWHONN Standards for Professional Fetal Monitoring Practice; TeamSTEPPS principles.
NEW QUESTION # 38
Usually, the duration of an early deceleration in comparison with the contraction is:
- A. Shorter
- B. The same
- C. Longer
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
An early deceleration is defined by NICHD and NCC as a gradual decrease and return of the fetal heart rate associated with uterine contractions. NCC emphasizes that early decelerations are:
* Symmetrical
* Uniform in shape
* Mirror images of the contraction
This means:
* Onset of deceleration = onset of contraction
* Nadir of deceleration = peak of contraction
* Recovery = end of contraction
* Duration of the deceleration # duration of the contraction
Thus, the correct answer is C. The same.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; NICHD Definitions; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing.
NEW QUESTION # 39
The tracing shown is a:
- A. Category I
- B. Category II
- C. Category III
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References (No URLs):
Interpretation of fetal heart rate (FHR) tracings in the NCC C-EFM exam follows the standardized NICHD three-tier classification, which is fully adopted in NCC's content outline and recommended references such as AWHONN Fetal Heart Monitoring Principles & Practices, Miller's EFM Pocket Guide, Menihan, Simpson' s Perinatal Nursing, and Creasy & Resnik.
Baseline:
The tracing demonstrates an FHR baseline around 145-150 bpm, which falls within the normal range of 110-
160 bpm. NCC references define baseline as the mean FHR rounded to increments of 5 bpm over a 10-minute window.
Variability:
The strip shows minimal variability, with amplitude fluctuations approximately 0-2 bpm.
According to NCC-aligned definitions:
* Moderate variability: 6-25 bpm
* Minimal variability: 1-5 bpm
* Absent variability: undetectable amplitude
This tracing shows minimal variability, not moderate, so it cannot be Category I.
Accelerations:
No accelerations are present. Lack of accelerations alone does not classify the tracing as Category III.
Decelerations:
There are no recurrent late decelerations, no recurrent variable decelerations, and no prolonged decelerations. Without these, and with minimal variability, the tracing does not meet Category III criteria.
Category III criteria (per NICHD/NCC):
Must include at least one of the following:
* Absent variability with recurrent late decelerations
* Absent variability with recurrent variable decelerations
* Absent variability with bradycardia
* Sinusoidal pattern
None of these are present.
Category II criteria (per NICHD/NCC):
Category II includes tracings that are not Category I or III.
Examples specifically listed include:
* Minimal variability
* Absent accelerations after fetal stimulation
* Tachycardia
* Bradycardia without absent variability
* Variable or late decelerations occurring intermittently
Because this tracing shows minimal variability, a normal baseline, no accelerations, and no recurrent decelerations, it fits squarely into Category II.
Therefore, the correct classification is Category II.
References:NCC C-EFM Candidate Guide and Content Outline (2025); AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine; NICHD Three-Tier FHR Interpretation System.
NEW QUESTION # 40
A woman (G1, P0) at 41-weeks gestation presents to OB triage to rule out labor. Her cervical exam is 1 cm/50%/-2. Membranes are intact. She would like to go home if not in labor. Based on this tracing, which represents the last two hours, the best approach is: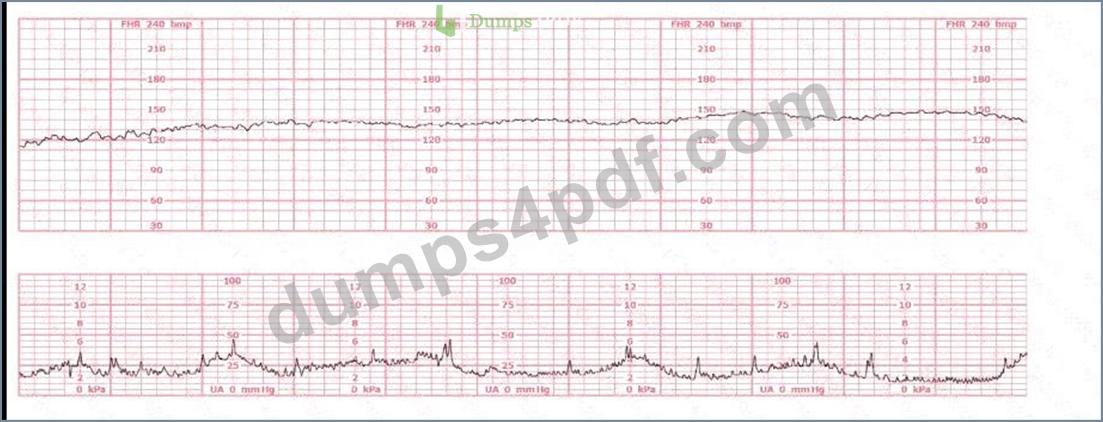
- A. further observation
- B. admission to hospital
- C. discharge to home
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources The fetal heart rate tracing shows a normal baseline (120-150 bpm), moderate variability, and no decelerations, consistent with a Category I pattern. According to AWHONN's Fetal Heart Monitoring Principles & Practices and NCC Perinatal Safety recommendations, a Category I tracing reliably indicates normal fetal acid-base status at the time of assessment and is considered reassuring.
Simpson & Creehan emphasize that in triage, management decisions depend on cervical status, contraction pattern, membrane status, and fetal well-being. With a cervix at 1 cm/50%/-2, intact membranes, and no regular labor pattern, she is not in active or latent labor requiring admission, provided fetal status is reassuring.
Menihan states that a normal tracing lasting two hours with moderate variability supports safe discharge when maternal and fetal assessments are normal. Creasy & Resnik confirm that reassuring fetal testing plus absence of labor is appropriate for outpatient management.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesSimpson & Creehan - Perinatal NursingMenihan
- Electronic Fetal MonitoringCreasy & Resnik - Maternal-Fetal MedicineMiller's Pocket Guide
NEW QUESTION # 41
(Full question)
This tracing would be categorized as a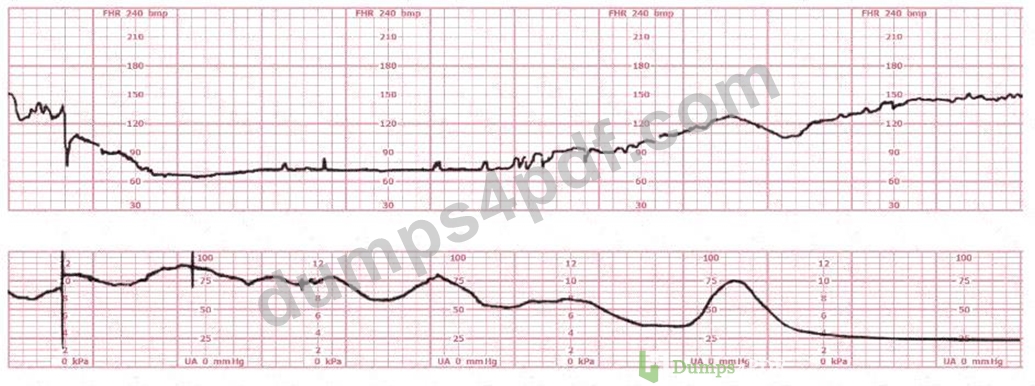
- A. Category I
- B. Category II
- C. Category III
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract (No URLs):
According to AWHONN Fetal Heart Monitoring Principles & Practice, Simpson & Miller, and the NCC C-EFM Content Outline, fetal heart rate categories are assigned based on baseline, variability, presence
/absence of accelerations, and type of decelerations.
A Category II tracing includes any pattern that is not clearly normal (Category I) or clearly abnormal (Category III). Classic Category II features include:
* Bradycardia NOT accompanied by absent variability
* Tachycardia
* Minimal variability
* Marked variability
* Absence of accelerations after stimulation
* Recurrent variable decelerations with minimal or moderate variability
* Prolonged decelerations (#2 min but <10 min)
In this tracing, the fetus demonstrates:
- A prolonged deceleration with subsequent recovery,
- Presence of baseline variability,
- Return toward baseline but not immediately normal.
AWHONN and Simpson state that any prolonged deceleration automatically places the tracing in Category II unless variability is absent (which would escalate it to Category III). Because variability is present, it cannot be Category III.
Therefore, by NCC standards, this tracing is Category II.
NEW QUESTION # 42
A fetal heart rate pattern shows no accelerations or decelerations. It would be interpreted as a Category II pattern if it occurred with:
- A. Marked variability
- B. A sinusoidal pattern
- C. A fetal heart rate of 110 beats per minute
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NICHD Category II includes:
* Minimal variability
* Marked variability
* Absent accelerations without recurrent decelerations
* Indeterminate baseline characteristics
A tracing with no accelerations and no decelerations becomes Category II if paired with marked variability, because marked variability indicates potential stress.
Why other answers are wrong:
* A. FHR 110 bpm # normal baseline if variability normal.
* B. Sinusoidal pattern # Category III, not Category II.
Correct answer: Marked variability.
References:NCC Candidate Guide; NICHD FHR Definitions; AWHONN FHMPP; Menihan.
NEW QUESTION # 43
The fetal heart rate tracing shown represents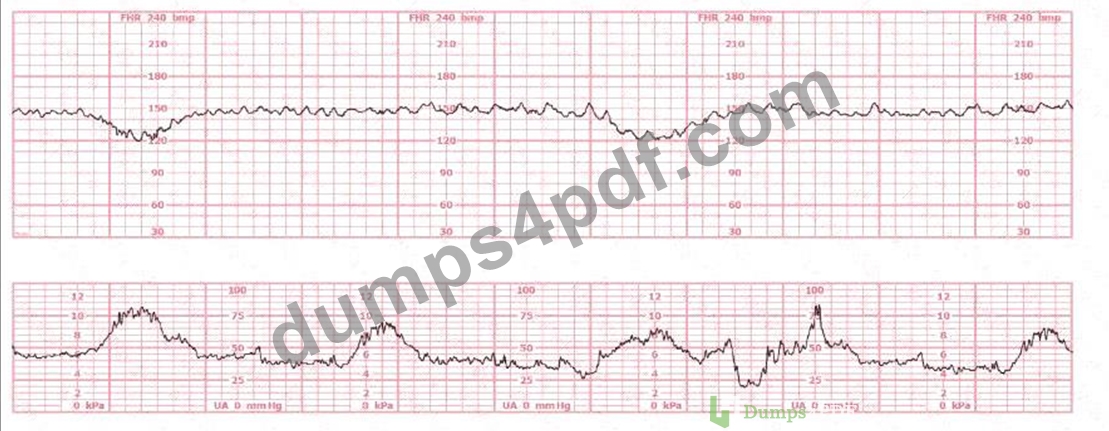
- A. category I
- B. category III
- C. category II
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources The tracing demonstrates a baseline within normal limits, moderate variability, and recurrent variable decelerations associated with contractions. According to NICHD/NCC definitions reproduced in AWHONN' s Fetal Heart Monitoring Principles & Practices and Menihan's Electronic Fetal Monitoring, recurrent variable decelerations with preserved variability classify the tracing as Category II.
A Category I pattern must show baseline 110-160, moderate variability, and absence of late or variable decelerations. Because this tracing shows recurrent variable decelerations, it does not meet Category I criteria.
Category III requires absent variability PLUS recurrent late decelerations, recurrent variable decelerations, bradycardia, or a sinusoidal pattern. This tracing shows moderate variability, therefore it cannot be Category III.
Simpson & Creehan emphasize that variable decelerations reflect cord compression and fall into Category II unless accompanied by absent variability. Miller's Pocket Guide confirms that moderate variability maintains fetal compensatory reserve, keeping the pattern in Category II.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesMenihan - Electronic Fetal MonitoringSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMiller's Pocket Guide
NEW QUESTION # 44
......
EFM exam questions for practice in 2026 Updated 127 Questions: https://pass4sure.dumps4pdf.com/EFM-valid-braindumps.html